


 Sign Out
Sign Out
Injection: Mechanism of Action: The bactericidal action of cefuroxime results from inhibition of cell wall synthesis by binding to essential target protein. Cefuroxime has bactericidal activity against a wide range of common pathogens, including beta-lactamase-producing strains and consequently is active against many ampicillin-resistant or amoxicillin-resistant strains.
Pharmacokinetics: Tablet: The bioavailability of cefuroxime axetil after oral administration is variable and depends on the formulation used. The tablet/capsule formulations should not, therefore be substituted with powder for oral suspension formulations on a mg/mg basis.
The bioavailability of cefuroxime axetil is significantly increased from 37% to 52% by coadministration with food.
Average peak serum of cefuroxime concentrations of 4.1, 7, or 13.6 mcg/mL are attained approximately 2 to 3 hours after oral administration in adults of a single 250 mg, 500 mg or 1 g dose, respectively. Average serum concentrations after 6 hours are 0.7, 2.2, or 3.4 mcg/mL, respectively. The area under the curve (AUC) of the drug averaged 12.9, 27.4, or 50 mcg-hr/mL, respectively.
Cefuroxime's apparent volume of distribution in healthy adult ranges from 9.3 to 15.8 L per 1.73 m2. The drug is 33-50% protein-bound. Cefuroxime readily crosses the placenta and can also be detected in human milk.
After oral administration of cefuroxime axetil, the drug undergoes rapid hydrolysis by nonspecific esterases in the intestinal mucosa and blood to yield the active parent drug cefuroxime, which is released into the systemic circulation. The axetil moiety of the drug is metabolized to acetaldehyde and acetic acid. Cefuroxime itself is not metabolized and its serum level is much closer to the minimum inhibitory concentration (MIC) of important pathogens than cefuroxime axetil.
Cefuroxime is excreted unchanged primarily in the urine by both glomerular filtration and tubular secretion.
In adults, the serum plasma half-life (t1/2) after oral administration of cefuroxime axetil ranges from 1.2 to 1.6 hours and about 50% of an administered dose is recovered in the urine within 12 hours.
In patients with renal impairment, the serum t1/2 of the drug is prolonged and generally ranges from 1.9-16.1 hours depending on the degree of renal impairment.
Injection: The sodium salt is given by intramuscular or intravenous injection. Peak plasma concentrations of about 27 micrograms/mL have been achieved 45 minutes after an intramuscular dose of 750 mg with measurable amounts present 8 hours after a dose. Up to 50% of cefuroxime in the circulation is bound to plasma proteins. The plasma half-life is about 70 minutes and is prolonged in patients with renal impairment and neonates.
Cefuroxime is widely distributed in the body including pleural fluid, sputum, bone, synovial fluid, & aqueous humour, but only achieves therapeutic concentrations in the CSF when the meninges are inflamed. It crosses the placenta and has been detected in breast milk.
Cefuroxime is excreted unchanged, by glomerular filtration and renal tubular secretion, and high concentrations are achieved in the urine. Following injection, most of a dose of cefuroxime is excreted within 24 hours, the majority within 6 hours. Probenecid competes for renal tubular secretion with cefuroxime resulting in higher and more prolonged plasma concentrations of cefuroxime. Small amounts of cefuroxime are excreted in bile.
Plasma concentrations are reduced by dialysis.
Microbiology: Tablet: Antimicrobial Spectrum of Activity: Cefuroxime has demonstrated against most strains of the following microorganisms both in vitro and in clinical infections: See Table 1.
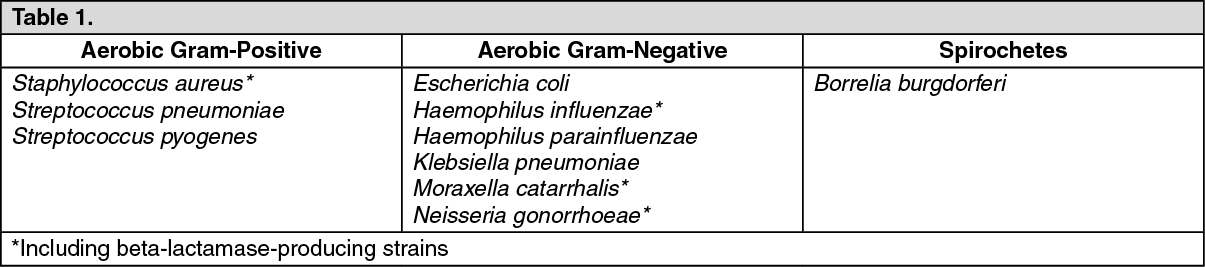 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCefuroxime has also demonstrated in vitro activity against most strains of the following microorganism; however, clinical significance is unknown: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageListeria monocytogenes and certain strains of enterococci, e.g., Enterococcus faecalis (formerly Streptococcus faecalis), are resistant to cefuroxime. Methicillin-resistant staphylococci are resistant to cefuroxime.
Pseudomonas spp., Campylobacter spp., Acinetobacter calcoaceticus, Legionella spp., and most strains of Serratia spp. and Proteus vulgaris are resistant to most first- and second-generation cephalosporins. Some strains of Morganella morganii, Enterobacter cloacae, and Citrobacter spp. have been shown by in vitro tests to be resistant to cefuroxime and other cephalosporins.
Most strains of Clostridium difficile and Bacteroides fragilis are resistant to cefuroxime.
Injection: Cefuroxime is usually active against the following organisms in vitro: Aerobes Gram-negative: Escherichia coli, Klebsiella spp., (including ampicillin-resistant strains), (including ampicillin-resistant strains), Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae (including penicillinase and non-penicillinase producing strains), Neisseria meningitides, Salmonella spp.
Aerobes Gram-positive: Staphylococcus aureus and Staphylococcus epidermidis (including penicillinase-producing strains but excluding methicillin-resistant strains), Streptococcus mitis (viridans groups), Bordetella pertussis.
Anaerobes: Gram-positive and Gram-negative cocci (including Peptococcus and Peptostreptococcus species). Gram-positive bacilli (including most Clostridium species) and Gram-negative bacilli (including Bacteroides and Fusobacterium species), Propionibacterium spp.
Other organisms: Borrelia burgdorferi.
The following organisms are not susceptible to cefuroxime: Clostridium difficile, Pseudomonas spp., Campylobacter spp., Acinetobacter calcoaceticus, Listeria monocytogenes, methicillin-resistant strains of Staphylococcus epidermidis, Legionella spp.
Some strains of the following genera are not susceptible to cefuroxime: Enterococcus (Streptococcus) faecalis, Morganella morganii, Proteus vulgaris, Enterobacter spp., Citrobacter spp., Serratia spp., Bacteroides fragilis.